
Itching between the toes is a surprisingly common issue—often dismissed as minor irritation—but when it lingers, it’s usually a sign of athlete’s foot (tinea pedis), a contagious fungal infection affecting up to 15% of the global population. While dry skin, eczema, or insect bites can also trigger toe itching, athlete’s foot is by far the most frequent cause, especially in warm, moist environments like sweaty shoes or public showers. Left untreated, this condition can lead to cracked, painful skin, bacterial infections, and even spread to toenails or other body parts. This guide dives deep into why athlete’s foot causes intense itching, how it spreads, and what sets it apart from similar-looking conditions. You’ll learn how to recognize early signs, avoid misdiagnosis, treat effectively, and prevent recurrence—so you can stop the itch and keep your feet healthy.
Fungal Infection Behind the Itch
Why Athlete’s Foot Causes Itching
Athlete’s foot isn’t just a rash—it’s a fungal invasion of the outer layer of skin. The culprits are dermatophytes, a group of fungi that feed on keratin, a protein found in your skin, hair, and nails. These organisms thrive in the warm, dark, and moist spaces between your toes—especially the gap between the fourth and fifth toes—where sweat gets trapped and airflow is minimal. As the fungi multiply, they secrete enzymes called keratinases that break down skin cells. This damage triggers your body’s immune response, causing inflammation, redness, and intense itching (pruritus). The longer the infection goes untreated, the worse the symptoms become, making scratching almost irresistible—and potentially spreading the fungus elsewhere.
Key Fungi Responsible
Three main types of dermatophytes cause athlete’s foot:
- Trichophyton rubrum – The most common, responsible for chronic, scaly infections with mild to moderate itching.
- Trichophyton mentagrophytes – Often leads to more aggressive symptoms, including blisters and acute inflammation.
- Epidermophyton floccosum – Less frequent but known to affect the web spaces and soles.
These fungi naturally live on human skin but only become problematic when conditions allow overgrowth. Once established, they can survive on shoes, socks, towels, and bathroom floors for weeks or even months, making reinfection easy if preventive steps aren’t taken.
Early vs. Advanced Symptoms
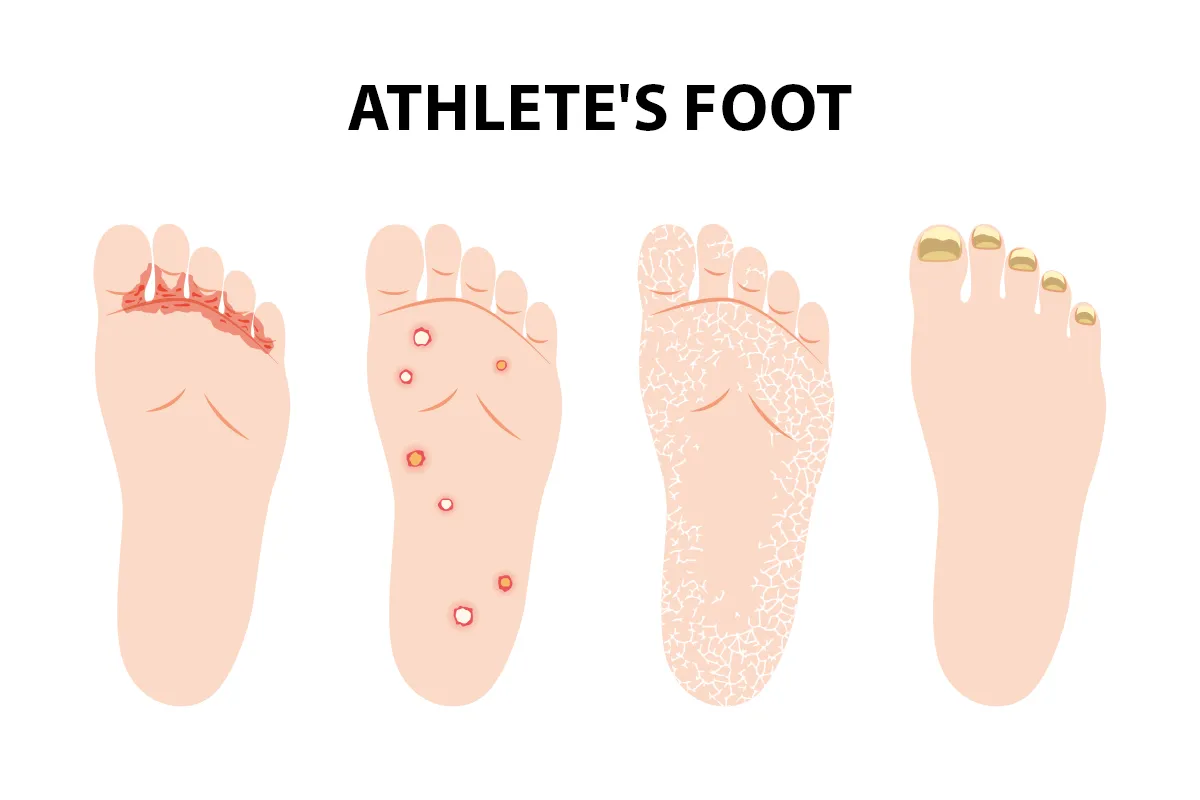
Early Signs of Infection
At first, athlete’s foot may be subtle and easily mistaken for dry skin:
- Slight flaking or peeling between the toes
- Mild itching, especially after removing shoes or socks
- No pain or odor in the beginning
- Skin may appear whitish, soggy, or macerated due to trapped moisture
Because symptoms start so mildly, many people ignore them. But without treatment, the infection progresses rapidly.
When It Gets Worse
As the fungus spreads, symptoms intensify:
- Itching becomes constant and unbearable
- Skin cracks or splits, sometimes bleeding
- Blisters may form and ooze fluid
- Redness, burning, and stinging increase
- A foul odor develops due to secondary bacterial growth in broken skin
If unchecked, the infection can spread to the soles (moccasin-type tinea pedis), toenails (onychomycosis), or even to the hands and groin through self-touch.
How Athlete’s Foot Spreads

Contagious in Public Places
Athlete’s foot is highly contagious and spreads easily in shared, damp environments:
- Walking barefoot in gyms, locker rooms, public showers, or pool decks
- Using contaminated towels, socks, or shoes
- Sharing foot mats, nail clippers, or shower floors
Fungal spores can survive on surfaces like tiles, carpets, and shoes for over 12 weeks. One study found infectious spores still active after more than three months on common household materials.
Autoinoculation: Spreading It Yourself
You can spread the fungus to other parts of your body just by touching infected skin:
- Scratching your toes, then touching your hands or groin
- Drying your feet with a towel used on other body areas
This often leads to:
– Tinea manuum (fungal hand infection)
– Tinea cruris (jock itch)
– Onychomycosis (fungal nail infection)
Always wash your hands thoroughly after touching infected skin and use a dedicated towel for your feet.
Risk Factors You Can Control
Sweaty Feet and Tight Shoes
Moisture is the #1 risk factor. Feet that sweat heavily or stay enclosed in non-breathable footwear—like rubber boots or plastic sneakers—create a perfect fungal breeding ground. Synthetic socks that trap sweat make it worse.
Prevention tip: Wear moisture-wicking socks (cotton, wool, or technical blends) and ventilated shoes made of leather or mesh.
Poor Drying Habits
Failing to dry between your toes after showering or swimming is a major contributor. Even a few minutes of dampness can kickstart fungal growth.
Pro move: Use a hairdryer on cool setting to fully dry toe webs, or gently pat with a paper towel.
Shared Spaces and Items
Using communal facilities without protection increases exposure:
- No shower shoes in gyms or dorms
- Sharing socks, shoes, or towels with others
Always wear waterproof sandals in public showers and never borrow footwear.
Medical Conditions That Raise Risk
Certain health issues make athlete’s foot more likely and harder to treat:
- Diabetes – Slower healing and higher infection risk
- Weakened immune system – From HIV, chemotherapy, or immunosuppressants
- Peripheral artery disease – Reduces blood flow to feet
- Eczema or psoriasis – Damaged skin lets fungi invade easier
If you have any of these, seek medical advice early—don’t rely solely on over-the-counter treatments.
Conditions That Mimic Athlete’s Foot

Dyshidrotic Eczema: Blisters and Itch
This form of eczema causes tiny, deep blisters on toes and soles, often triggered by stress or sweaty feet. Unlike athlete’s foot:
– Blisters are itchy but not scaly
– Doesn’t respond to antifungals
– May flare seasonally
Using antifungal cream on eczema can worsen irritation. A dermatologist can confirm the diagnosis with a skin test.
Shoe Contact Dermatitis: Allergic Reaction
Some people react to chemicals in shoes—like rubber, dyes, or adhesives. Symptoms include:
– Red, itchy rash where shoes touch skin
– Often worse on top of feet or heels
– Improves when switching footwear
A 2007 study found rubber accelerators and resins are common allergens. Patch testing can identify the trigger.
Insect Bites: Fleas, Mites, Chiggers
Bug bites can resemble fungal rashes:
– Flea bites often appear in groups of three (“breakfast, lunch, dinner”)
– Chigger bites cause intense itching on ankles and toes
– Mosquito bites are larger, puffy, and temporary
These usually resolve with antihistamines or hydrocortisone, not antifungals.
Hookworm Infection: Travel-Related Rash
Rare in the U.S., but possible after walking barefoot in tropical areas with contaminated soil. Hookworm larvae burrow into skin, causing:
– Serpiginous (snake-like) rash
– Intense itching
– May lead to diarrhea or abdominal pain
Requires antiparasitic medication, not antifungals.
Other Look-Alike Conditions
- Psoriasis: Thick, red patches with silvery scales
- Allergic dermatitis: Reaction to soaps or detergents
- Chilblains: Red, itchy patches from cold exposure
Key takeaway: If OTC antifungals don’t work after 2 weeks, see a doctor. Misdiagnosis delays healing.
Diagnosis: How Doctors Confirm It
Visual Clues Doctors Look For
Most cases are diagnosed by appearance:
– Scaling and maceration between toes
– Redness and peeling in web spaces
– Dry, scaly soles in moccasin-type infections
But because many conditions look alike, testing may be needed.
Lab Tests for Confirmation
- KOH (potassium hydroxide) test: A skin scraping is treated with KOH and examined under a microscope for fungal hyphae. Results in minutes.
- Fungal culture: Skin sample is grown in a lab to identify the exact fungus. Takes 2–4 weeks, useful for stubborn cases.
- Biopsy: Rarely used, only if diagnosis is unclear or infection is severe.
These tests rule out eczema, psoriasis, or bacterial infections.
Treatment That Works
Topical Antifungals: First Choice
Over-the-counter creams and sprays kill the fungus:
– Terbinafine (Lamisil) – Most effective, fungicidal (kills fungi)
– Clotrimazole (Lotrimin) – Broad-spectrum, widely available
– Miconazole (Micatin) – Good for mild cases
– Butenafine (Mentax) – Works fast, once-daily use
– Tolnaftate – Less effective but affordable
How to apply:
1. Wash and dry feet completely
2. Apply cream to affected area and 1 inch beyond
3. Use twice daily for 2–6 weeks
4. Continue 1–4 weeks after symptoms disappear to prevent relapse
Sprays and powders help keep feet dry and prevent reinfection.
Oral Medications for Severe Cases
Prescribed when:
– Infection is widespread or resistant
– Toenails are infected
– Topicals fail
Common options:
– Terbinafine – 90% cure rate, taken for 2–6 weeks
– Itraconazole – Pulse dosing (1 week on, 3 weeks off)
– Fluconazole – Weekly dosing, less effective
Warning: These can affect the liver. Blood tests are often required before and during treatment.
Soaks and Adjunct Treatments
- Burow’s solution (aluminum subacetate): Soak feet 20 minutes twice daily to dry out soggy skin
- Antibiotics: Needed if cellulitis develops (swelling, pus, fever)
- Topical steroids (short-term): Reduce inflammation when combined with antifungals—never use alone
Home Remedies: What Works?
- Tea tree oil: A 2002 study showed 50% improvement in some cases, but not as effective as terbinafine
- Neem oil: Traditional remedy with antifungal properties (2015 study support)
Reality check: These may help mild cases but should not replace proven treatments for active infections.
Preventing Recurrence
Daily Foot Hygiene Must-Dos
- Wash feet daily with soap and water
- Dry thoroughly, especially between toes
- Use a dedicated foot towel or disposable wipes
- Moisturize dry skin—but avoid between toes
Smart Footwear Choices
- Wear breathable shoes (leather, mesh)
- Choose cotton or wool socks that wick moisture
- Change socks daily or after sweating
- Rotate shoes—let each pair dry for 24–48 hours
- Disinfect shoes with antifungal sprays or UV devices
Public Area Protection
- Never walk barefoot in locker rooms, pools, or gyms
- Wear flip-flops or shower shoes in public showers
- Avoid sharing towels, socks, shoes, or nail tools
Household Decontamination
If someone in your home has athlete’s foot:
– Wash towels and sheets in hot water
– Disinfect bathroom floors and mats
– Use antifungal spray on carpets, rugs, and shower stalls
When to See a Doctor
Red Flags Needing Medical Care
Seek help if:
– No improvement after 2 weeks of OTC treatment
– Skin is cracked, oozing, or painful
– Signs of infection: redness spreading, warmth, pus, fever
– You have diabetes or a weakened immune system
– Infection spreads to nails, hands, or groin
– Walking becomes difficult
Immediate care is needed for cellulitis, which can become life-threatening.
Special Advice for High-Risk Groups
- Diabetics: Even small cracks can lead to ulcers. See a doctor at the first sign.
- Immunocompromised: Infections can spread deeper. Early treatment is critical.
- Elderly: Slower healing increases complication risk.
Final Note: Athlete’s foot is common but not harmless. Left untreated, it can lead to serious complications—especially in people with diabetes or weak immune systems. The key to success is early action, correct diagnosis, and consistent treatment. Don’t guess—when in doubt, see a podiatrist or dermatologist. With the right care, you can stop the itch and keep your feet healthy year-round.